
 Tweet
Tweet
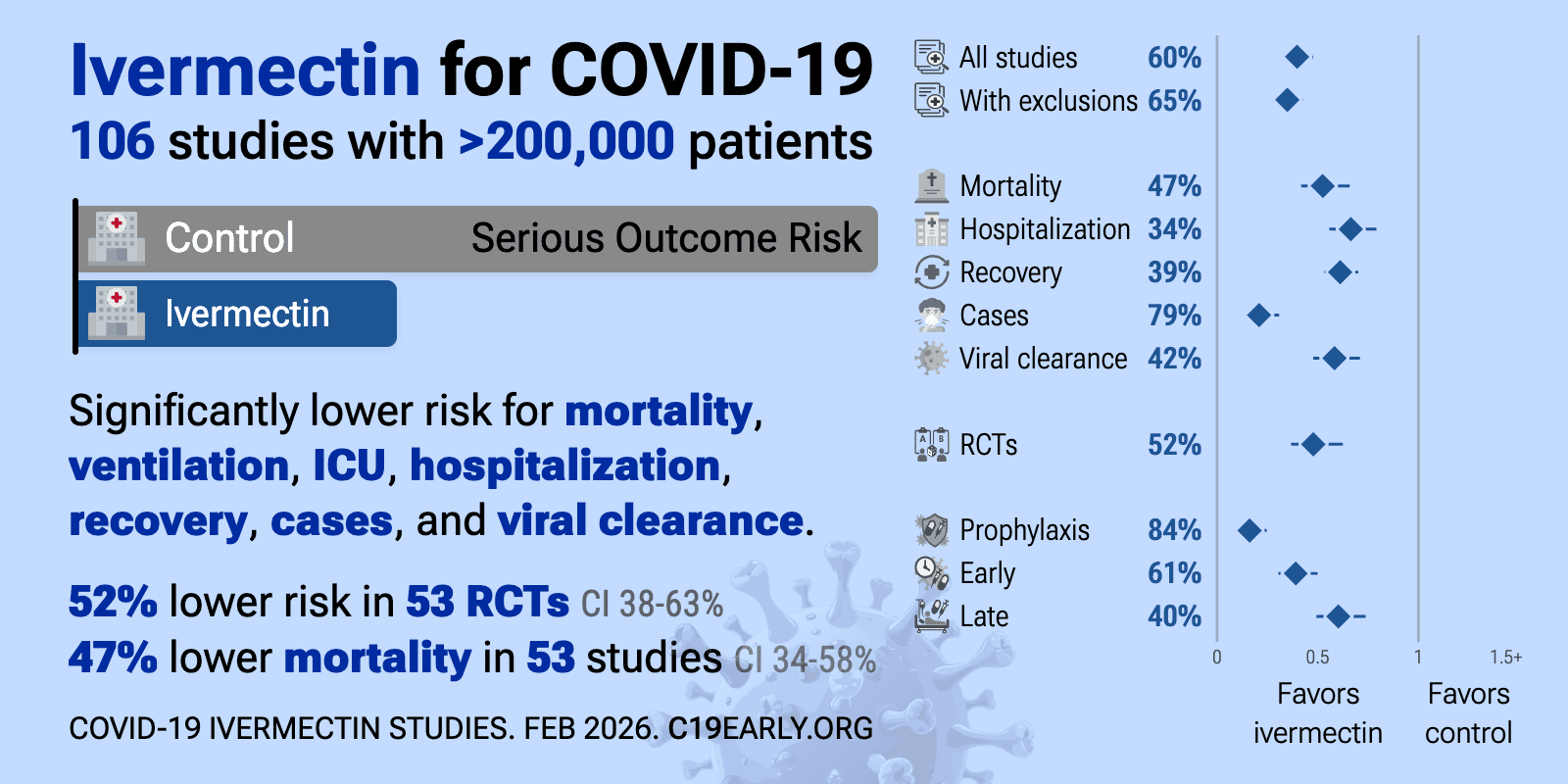
Hospitalizations, Mortality Cut In Half After Brazilian City Offered Ivermectin To Everyone Pre-Vaccine
-
-
Anyone know the cost of 3 jabs? How much does this cost the us government and later the taxpayersRule 1- ALL GUNS ARE ALWAYS LOADED
Rule 2 -NEVER LET THE MUZZLE COVER ANYTHING YOU ARE NOT PREPARED TO DESTROY (including your hands and legs)
Rule 3 -KEEP YOUR FINGER OFF THE TRIGGER UNTIL YOUR SIGHTS ARE ON THE TARGET
Rule 4 -BE SURE OF YOUR TARGET AND WHAT IS BEYOND IT
(thanks to Jeff Cooper) -
Can’t be true… horse paste doesn’t work, or so we’ve been told.MAGA - drain the swamp^D^D^D^D^Dcesspool!
Proud deplorable wacist!
#NotMyStateGovernment!
Just remember BAMN - there is no level too low for them to stoop!
COVID survivor - ain?t gonna get pricked!Comment
-
What do you call the people that abandoned the agenda of John Kennedy and adopted the agenda of Lee Oswald?
Pronouns: "Dude" and "Playa".
https://billstclair.com/Unintended-Consequences.pdf
I was born under a wandrin star.Comment
-
Que the Rocket de-bunking.Originally posted by tonelarComment
-
Crazy isn't it?
they carry the memes and fake news stories about horse paste that they were sent out with thinking they are some kind of kill shot but have no qualms about taking multiple injections of a substance that has passed neither animal or human trials.Last edited by stonefly-2; 12-13-2021, 8:40 AM.What do you call the people that abandoned the agenda of John Kennedy and adopted the agenda of Lee Oswald?
Pronouns: "Dude" and "Playa".
https://billstclair.com/Unintended-Consequences.pdf
I was born under a wandrin star.Comment
-
Hmm. Interesting paper, big claims. I have questions.
The first is purely mechanical. I was able to find the original, and it claims to be a preprint -- but I can't find the journal that is publishing or reviewing it. This is strange. Also strange is the fact that this paper is a whole yearwidely panned in the press, but these are opinion pieces. Could it have worked? What is the evidence?
This new paper, led by individuals such as Dr. Lucy Kerr who were early supporters of ivermectin, at a time when most of us were distracted by hydroxychloroquine , has two findings: First, a barely noticeable but significant reduction in infections in the ivermectin-using community, and second, a much stronger reduction in fatalities from the disease. This effect is so strong that it should be very easy to replicate, if it is real.
So why was it not seen before? Why did it take a whole year after the program concluded to report on this result? Brazil was hardly free of the virus after December 2020; indeed, they were on the upswing at that point, reaching a maximum in April 2021 at almost three times the previous high-water mark. I have some ideas.
The biggest problem with this paper is that there were essentially no controls. This is not a blinded study -- it is also supposed that access to the treatment was even across the whole population, but that's almost impossible to achieve in practice.Originally posted by Kerr et al.
The risk is that the population opting for ivermectin and the population abstaining or denied access are different and, most importantly, behave differently. And there are clear signs of this in the population data collected after the fact. Table 1 shows the difference very clearly: The "control" population has a higher fraction of subjects under 30 years old (27.8% vs. 20.5%) and a much lower fraction of subjects over 50 years old (20.0% vs. 30.5%). You wouldn't see this with a placebo-controlled trial.
"Aha, but the control group, being younger, should have had a lower mortality rate -- and they didn't," the paper points out. Well, maybe. But there are some other curious artifacts in the results.
The rate of infection is apparently estimated from a single PCR test. This result was also the gate used to include or exclude participants from this analysis:
59% of hospitalized cases eventually died, and in the control group, that number went up to 62%.Originally posted by Kerr et al.
How can we explain these numbers? This isn't anything like the USA, where hospitalized CFR is about 10 - 15%. It's also well out of family for Brazil, which reported 31.8% to 18.2% over the period of interest.
There is no good explanation for this, and it's because the study is lacking in detail. We don't actually know what fraction of mortal cases were hospitalized. In this country, unhospitalized fatalities are rare, but based on the figures above, it is plausible that half or more of those in this study occurred outside of the hospital.
And that's a problem. Because this study only monitored its subjects at the point of care, mortality too ceases to be a reliable signal. The paper provides no consideration of control for these sampling problems.
Were the COVID-19 deaths overcounted? This is unknown, but there is some evidence supporting this. , 58% higher than the state average. But alternately, the counts might indeed be accurate, caused instead by some unknown peculiarity in the city. Past criticism of the ivermectin study has pointed out that the ivermectin experiments do not appear to have lowered overall cases or deaths -- indeed, the opposite is true -- but with additional information, it looks to be an artifact.
What most catches my attention, however, is that the CFR was not at all uniform in time. From the paper, over the period of July 7, 2020 to December 31, 2020, there were 7,345 cases with 141 fatalities, for a CFR of 1.9%. But they didn't pay any attention to stability of this signal.
Fatalities, but not cases, were front-loaded, with 2,882 cases and 99 deaths between July 7 and August 23, leaving 4,463 cases but only 42 fatalities from August 23 and December 31. So before the August 23 breakpoint, the CFR was 3.44%, whereas afterward, it fell to 0.94%. This applies to the whole sample -- and this is a far more statistically significant result than the ivermectin vs. untreated comparison.
August 23 may have marked a significant change in behavior. It's a fuzzy date, but clearly dynamics were different on both sides of that date. But it had nothing to do with ivermectin. Until this artifact is understood, we have no reason to suspect the data analysis in this paper is valid.
Now: This finding does not falsify the paper. A more thorough analysis might recover the conclusion of this paper, if, for instance, the relative risk between ivermectin and control is preserved on both sides of the August 23 boundary.
But until this is done, we can have no confidence in their conclusion. Something happened in August that changed the progression of the pandemic in this location. I will speculate that it represents a behavioral change, possibly driven by seasonality, and probably exposing very different demographic groups to the virus. Another possibility is that the results are skewed by an early pulse hitting seniors, with those in group care settings both less likely to reach medical supplies and more likely to perish, until this population was largely depleted by mid-August, when counts nationwide began to drop. Still a third possibility is undercounting of cases prior to August 23, with more tests being available afterward -- but if this is causing such a large artifact, our CFR is essentially invalid for the whole experiment.
I don't know what's going on with these data. It will take more study. But we can draw two conclusions:- The statistical significance of ivermectin in these data is greatly overshadowed by a different discriminator, and therefore, concluding ivermectin had a causative effect is premature; and
- I was able to make this determination at a distance in a matter of hours, and it is surprising that the researchers did not consider such an obvious confound.
--
I would love for ivermectin to be effective. If it is, it should be easy to demonstrate -- but it hasn't been. This study is a good illustration of why controls are important. More detail may yet save this conclusion, but I predict that it won't be provided, given they've been sitting on it for a year.Riflemen Needed.
Ask me about Appleseed! Send a PM or see me in the Appleseed subforum.Comment

There are currently 7594 users online. 127 members and 7467 guests.
Most users ever online was 239,041 at 10:39 PM on 02-14-2026.









Comment